Learn How To Treat Severs Disease?
Overview
Severs Disease is a common cause of heel pain in children. It is seen most commonly in children aged 5 - 11 years old. Children with Severs Disease will complain of heel pain that increases with activity. The pain is often relieved by rest, although some children will continue to have pain with regular activities, such as walking. Severs Disease has much in common with Osgood-Schlatter Disease. Both are described as being a traction apophysitis.
Causes
Risk Factors For Sever?s Disease. While anyone can get Sever?s Disease, it most commonly affects boys, but may also affect girls. Children ages eight to thirteen. Children involved in high-impact sports like baseball, football and soccer. Kids with forefoot to midfoot misalignment walking patterns. Poor-fitting shoes. Standing for long periods of time. Obesity. Flat feet. A gait that roll inwards.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
For patients suffering from Sever's disease, the pediatric orthopaedic surgeon will often recommend a conservative treatment plan including anti-inflammatory medication (as directed by the doctor). Application of ice to the heel. Calf, hamstring, and heel stretches. Orthotics. Modification of activities. There are rarely any complications with the treatment of Sever's disease, and symptoms generally resolve within 2 weeks to 2 months. Patients can typically return to playing sports again after the heel pain has resolved. The physician will let confirm when it is safe to resume physical activities.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Severs Disease is a common cause of heel pain in children. It is seen most commonly in children aged 5 - 11 years old. Children with Severs Disease will complain of heel pain that increases with activity. The pain is often relieved by rest, although some children will continue to have pain with regular activities, such as walking. Severs Disease has much in common with Osgood-Schlatter Disease. Both are described as being a traction apophysitis.
Causes
Risk Factors For Sever?s Disease. While anyone can get Sever?s Disease, it most commonly affects boys, but may also affect girls. Children ages eight to thirteen. Children involved in high-impact sports like baseball, football and soccer. Kids with forefoot to midfoot misalignment walking patterns. Poor-fitting shoes. Standing for long periods of time. Obesity. Flat feet. A gait that roll inwards.
Symptoms
Symptoms of Sever?s disease, mostly pain at the back of heel, usually occur during and after sporting activity, and usually disappear with rest. In some cases, children may find it difficult to place pressure on their heels, and begin walking on their toes to gain relief. For some children, the heel pain will persist until the next morning, causing some stiffness or hobbling on first arising. Some children may experience mild swelling at the back of the heel.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
For patients suffering from Sever's disease, the pediatric orthopaedic surgeon will often recommend a conservative treatment plan including anti-inflammatory medication (as directed by the doctor). Application of ice to the heel. Calf, hamstring, and heel stretches. Orthotics. Modification of activities. There are rarely any complications with the treatment of Sever's disease, and symptoms generally resolve within 2 weeks to 2 months. Patients can typically return to playing sports again after the heel pain has resolved. The physician will let confirm when it is safe to resume physical activities.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
What Are The Leading Causes Of Posterior Tibial Tendon Dysfunction ?
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot?s arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place. 
Causes
Obesity - Overtime if your body is carrying those extra pounds, you can potentially injure your feet. The extra weight puts pressure on the ligaments that support your feet. Also being over weight can lead to type two diabetes which also can attribute to AAFD. Diabetes - Diabetes can also play a role in Adult Acquired Flatfoot Deformity. Diabetes can cause damage to ligaments, which support your feet and other bones in your body. In addition to damaged ligaments, uncontrolled diabetes can lead to ulcers on your feet. When the arches fall in the feet, the front of the foot is wider, and outer aspects of the foot can start to rub in your shoe wear. Patients with uncontrolled diabetes may not notice or have symptoms of pain due to nerve damage. Diabetic patient don?t see they have a problem, and other complications occur in the feet such as ulcers and wounds. Hypertension - High blood pressure cause arteries narrow overtime, which could decrease blood flow to ligaments. The blood flow to the ligaments is what keeps the foot arches healthy, and supportive. Arthritis - Arthritis can form in an old injury overtime this can lead to flatfeet as well. Arthritis is painful as well which contributes to the increased pain of AAFD. Injury - Injuries are a common reason as well for AAFD. Stress from impact sports. Ligament damage from injury can cause the bones of the foot to fallout of ailment. Overtime the ligaments will tear and result in complete flattening of feet.
Symptoms
Most people will notice mild to extreme pain in their feet. Below outlines some signs and symptoms of AAFD. Trouble walking or standing for any duration. Pain and swelling on the inside of the ankle. Bump on the bottom of the foot. Ulcer or wound developing on the outer aspects of foot.
Diagnosis
There are four stages of adult-acquired flatfoot deformity (AAFD). The severity of the deformity determines your stage. For example, Stage I means there is a flatfoot position but without deformity. Pain and swelling from tendinitis is common in this stage. Stage II there is a change in the foot alignment. This means a deformity is starting to develop. The physician can still move the bones back into place manually (passively). Stage III adult-acquired flatfoot deformity (AAFD) tells us there is a fixed deformity. This means the ankle is stiff or rigid and doesn???t move beyond a neutral (midline) position. Stage IV is characterized by deformity in the foot and the ankle. The deformity may be flexible or fixed. The joints often show signs of degenerative joint disease (arthritis).
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found. 
Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.
What Can Cause Pain In The Foot's Arch ?
Overview
Arch pain (medically known as plantar pain) is a broad term many people use to describe pain in their muscles, tendons, ligaments, bones, or nerves. All these components are connected to the bottom of the foot; therefore, damage to any one of these can cause pain on the bottom of the foot. This pain may only last for short time, but can progressively worsen if untreated. Most people who suffer from this pain are between the ages of 30 and 80, but many younger athletes are also susceptible, particularly those who participate in high-impact sports.

Causes
Flat feet are a common condition. The condition is normal in infants and toddlers. Flat feet occur because the tissues holding the joints in the foot together (called tendons) are loose. The tissues tighten and form an arch as children grow older. This will take place by the time the child is 2 or 3 years old. Most people have normal arches by the time they are adults. However, the arch may never form in some people. Aging, injuries, or illness may harm the tendons and cause flat feet to develop in a person who has already formed arches. This type of flat foot may occur only on one side. Rarely, painful flat feet in children may be caused by a condition in which two or more of the bones in the foot grow or fuse together. This condition is called tarsal coalition.
Symptoms
Persistant pain and selling under the ball of the foot and extending towards the toes (most commonly the 2nd). Some swelling may be disable on the top of the foot along with redness. Often a sensation of 'walking on the bones for the foot' will be described, and there is a positive Lachman's test. Often a tear will result in the toes splaying (daylight sign) and clawing.
Diagnosis
In people with flat feet, the instep of the foot comes in contact with the ground when standing. To diagnose the problem, the health care provider will ask you to stand on your toes. If an arch forms,the flat foot is called flexible. You will not need any more tests or treatment. If the arch does not form with toe-standing (called rigid flat feet), or if there is pain, other tests may be needed, including a CT scan to look at the bones in the foot. MRI scan to look at the tendons in the foot. X-ray of the foot.
Non Surgical Treatment
The most effective treatment for foot arch pain and strain is to use an arch support. The arch support sits under the foot and stops the arch of the foot from collapsing, thereby preventing the stretch of the arch pad which causes pain and discomfort. Wearing an arch support in slippers or house shoes can also prevent pain in the mornings when discomfort it most common and severe. Arch supports usually relieve symptoms within a few days.

Surgical Treatment
In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground.
Prevention
Foot and ankle injuries are common in sports, especially running, tennis and soccer. But sports enthusiasts can decrease the risk of injury by taking some precautions. Lightly stretch or better yet, do a slow jog for two to three minutes to warm up the muscles. Don't force the stretch with a "bouncing motion." The amount of time spent on the activity should be increased gradually over a period of weeks to build both muscle strength and mobility. Cross training by participating in different activities can help build the muscles. People whose feet pronate or who have low arches should choose shoes that provide support in both the front of the shoe and under the arch. The heel and heel counter (back of the shoe) should be very stable. Those with a stiffer foot or high arches should choose shoes with more cushion and a softer platform. Use sport-specific shoes. Cross training shoes are an overall good choice; however, it is best to use shoes designed for the sport.
Stretching Exercises
Try these simple stretches to assist with relieving pain in your arches. (Note: Stretch slowly and gently. You should feel a moderate pull on the muscle and tendon but no pain. If these stretches are painful, stop and seek further advice from a health professional). STRETCH ONE. Stand at arm?s length from a wall with one foot in front of the other, forward knee bent. Keeping your back leg straight and back heel on the floor, lean into the wall until you feel a stretch in your calf. STRETCH TWO. This time, bend your back leg slightly, and lean into the wall. You should feel a stretch in the lower part of your calf. Hold each stretch for 20 seconds and repeat on each leg, a few times daily.
Arch pain (medically known as plantar pain) is a broad term many people use to describe pain in their muscles, tendons, ligaments, bones, or nerves. All these components are connected to the bottom of the foot; therefore, damage to any one of these can cause pain on the bottom of the foot. This pain may only last for short time, but can progressively worsen if untreated. Most people who suffer from this pain are between the ages of 30 and 80, but many younger athletes are also susceptible, particularly those who participate in high-impact sports.
Causes
Flat feet are a common condition. The condition is normal in infants and toddlers. Flat feet occur because the tissues holding the joints in the foot together (called tendons) are loose. The tissues tighten and form an arch as children grow older. This will take place by the time the child is 2 or 3 years old. Most people have normal arches by the time they are adults. However, the arch may never form in some people. Aging, injuries, or illness may harm the tendons and cause flat feet to develop in a person who has already formed arches. This type of flat foot may occur only on one side. Rarely, painful flat feet in children may be caused by a condition in which two or more of the bones in the foot grow or fuse together. This condition is called tarsal coalition.
Symptoms
Persistant pain and selling under the ball of the foot and extending towards the toes (most commonly the 2nd). Some swelling may be disable on the top of the foot along with redness. Often a sensation of 'walking on the bones for the foot' will be described, and there is a positive Lachman's test. Often a tear will result in the toes splaying (daylight sign) and clawing.
Diagnosis
In people with flat feet, the instep of the foot comes in contact with the ground when standing. To diagnose the problem, the health care provider will ask you to stand on your toes. If an arch forms,the flat foot is called flexible. You will not need any more tests or treatment. If the arch does not form with toe-standing (called rigid flat feet), or if there is pain, other tests may be needed, including a CT scan to look at the bones in the foot. MRI scan to look at the tendons in the foot. X-ray of the foot.
Non Surgical Treatment
The most effective treatment for foot arch pain and strain is to use an arch support. The arch support sits under the foot and stops the arch of the foot from collapsing, thereby preventing the stretch of the arch pad which causes pain and discomfort. Wearing an arch support in slippers or house shoes can also prevent pain in the mornings when discomfort it most common and severe. Arch supports usually relieve symptoms within a few days.
Surgical Treatment
In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground.
Prevention
Foot and ankle injuries are common in sports, especially running, tennis and soccer. But sports enthusiasts can decrease the risk of injury by taking some precautions. Lightly stretch or better yet, do a slow jog for two to three minutes to warm up the muscles. Don't force the stretch with a "bouncing motion." The amount of time spent on the activity should be increased gradually over a period of weeks to build both muscle strength and mobility. Cross training by participating in different activities can help build the muscles. People whose feet pronate or who have low arches should choose shoes that provide support in both the front of the shoe and under the arch. The heel and heel counter (back of the shoe) should be very stable. Those with a stiffer foot or high arches should choose shoes with more cushion and a softer platform. Use sport-specific shoes. Cross training shoes are an overall good choice; however, it is best to use shoes designed for the sport.
Stretching Exercises
Try these simple stretches to assist with relieving pain in your arches. (Note: Stretch slowly and gently. You should feel a moderate pull on the muscle and tendon but no pain. If these stretches are painful, stop and seek further advice from a health professional). STRETCH ONE. Stand at arm?s length from a wall with one foot in front of the other, forward knee bent. Keeping your back leg straight and back heel on the floor, lean into the wall until you feel a stretch in your calf. STRETCH TWO. This time, bend your back leg slightly, and lean into the wall. You should feel a stretch in the lower part of your calf. Hold each stretch for 20 seconds and repeat on each leg, a few times daily.
Achilles Tendon Rupture Long Leg Cast Photos
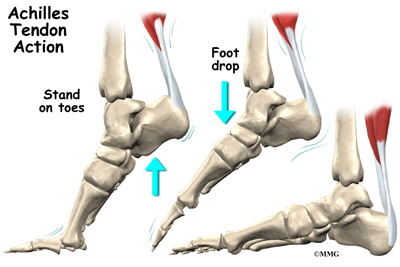
Overview  The Achilles tendon is the large cord like structure on the back of the leg just above the heel. It is the largest tendon in the body and has a tremendous amount of force transmitted through it during walking, running and jumping activities. The Achilles tendon is prone to injury, including rupture during periods of increased stress and activity. Common activities causing injury include running, basketball, baseball, football, soccer, volleyball and tennis. These activities require jumping and pushing forces that are possible due to the strength of the calf musculature and the ability of the Achilles tendon to endure this stress. Men from the ages of 30-50 are the most commonly injured during weekend athletic activities. Causes The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture. Symptoms Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis. Diagnosis Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Plain radiography. Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst, in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI). MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis. Non Surgical Treatment Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months.
The Achilles tendon is the large cord like structure on the back of the leg just above the heel. It is the largest tendon in the body and has a tremendous amount of force transmitted through it during walking, running and jumping activities. The Achilles tendon is prone to injury, including rupture during periods of increased stress and activity. Common activities causing injury include running, basketball, baseball, football, soccer, volleyball and tennis. These activities require jumping and pushing forces that are possible due to the strength of the calf musculature and the ability of the Achilles tendon to endure this stress. Men from the ages of 30-50 are the most commonly injured during weekend athletic activities. Causes The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture. Symptoms Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis. Diagnosis Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Plain radiography. Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst, in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI). MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis. Non Surgical Treatment Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months.  Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low. Prevention The following can significantly reduce the risk of Achilles tendon rupture. Adequate stretching and warming up prior to exercising. If playing a seasonal sport, undertake preparatory exercises to build strength and endurance before the sporting season commences. Maintain a healthy body weight. This will reduce the load on the tendon and muscles. Use footwear appropriate for the sport or exercise being undertaken. Exercise within fitness limits and follow a sensible exercise programme. Increase exercise gradually and avoid unfamiliar strenuous exercise. Gradual ?warm down? after exercising.
Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low. Prevention The following can significantly reduce the risk of Achilles tendon rupture. Adequate stretching and warming up prior to exercising. If playing a seasonal sport, undertake preparatory exercises to build strength and endurance before the sporting season commences. Maintain a healthy body weight. This will reduce the load on the tendon and muscles. Use footwear appropriate for the sport or exercise being undertaken. Exercise within fitness limits and follow a sensible exercise programme. Increase exercise gradually and avoid unfamiliar strenuous exercise. Gradual ?warm down? after exercising.
What Could Cause Achilles Tendonitis ?
Overview
 Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Causes
The two most common causes of Achilles tendonitis are Lack of flexibility and Overpronation. Other factors associated with Achilles tendonitis are recent changes in footwear, and changes in exercise training schedules. Often long distance runners will have symptoms of Achilles tendonitis after increasing their mileage or increasing the amount of hill training they are doing. As people age, tendons, like other tissues in the body, become less flexible, more rigid, and more susceptible to injury. Therefore, middle-age recreational athletes are most susceptible to Achilles tendonitis.
Symptoms
Mild ache in the back of the lower leg, especially after running. More acute pain may occur after prolonged activity, Tenderness or stiffness in the morning. In most cases the pain associated with Achilles tendinitis is more annoying than debilitating, making sufferers regret activity after the fact, but not keeping them from doing it. More severe pain around the Achilles tendon may be a symptom of a much more serious ruptured tendon.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
As with all conditions, your Doctor should be consulted. Even minor symptoms can represent significant damage to the Achilles tendon. It is recommended that medical advice be sought as soon as symptoms are experienced. Applying ice to the injury on a regular basis can reduce inflammation associated with Achilles Tendonosis. Following the initial injury, ice should be applied for periods of 15 minutes every hour. Resting the injured ankle may be necessary. This can be a problem for athletes who need to train regularly. The degree of rest required depends on the severity and type of Achilles Tendonosis. Your Health Care Professional will advise you about what activities should be limited while the injury is repairing. Fast uphill and downhill running is not advised while an Achilles Tendinosis injury is healing. Anti-inflammatory, analgesic medications such as those containing aspirin may help control pain and inflammation. Self-massage with heat-inducing creams and liniments may be of assistance. Wearing heel-lifts or pads in shoes can reduce the tension in the Achilles tendon. Physiotherapy may assist in the repair of a damaged Achilles tendon. Physiotherapists may recommend exercises to strengthen the tendon to reduce the chances of future injury. Regular stretching of the hamstring muscles (at the back of the calf) can help the repair process. This should only be done when the injury has repaired enough not to cause pain during this stretching. Taping the ankle and wearing appropriate running shoes may help to control movement in the ankle and prevent further injury.

Surgical Treatment
Chronic Achilles tendon tears can be more complicated to repair. A tendon that has torn and retracted (pulled back) into the leg will scar in the shortened position over time. Restoring normal tendon length is usually not an issue when surgery is performed within a few weeks of the injury. However, when there has been a delay of months or longer, the treatment can be more complicated. Several procedures can be used to add length to a chronic Achilles tear. A turndown procedure uses tissue folded down from the top of the calf to add length to the Achilles tendon. Tendon transfers from other tendons of the ankle can also be performed to help restore function of the Achilles. The results of surgery in a chronic situation are seldom as good as an acute repair. However, in some patients, these procedures can help restore function of a chronically damaged Achilles.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, icorporate stretching into your warm-up and cool-down routines. Maintaining an adequate level of fitness for your sport. Avoid dramatic increases in sports training. If you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse. Wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses. Avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury. Maintain a normal healthy weight.
Typically an overuse injury, Achilles tendinitis affects the connective tissue between the calf and the heel. When you walk, run or otherwise use your leg to push your body upward, the Achilles tendon is engaged. Using the tendon frequently and with high intensity often results in tendinitis -- a swollen Achilles tendon that makes it difficult and sometimes painful to continue high-impact activities.
Causes
The two most common causes of Achilles tendonitis are Lack of flexibility and Overpronation. Other factors associated with Achilles tendonitis are recent changes in footwear, and changes in exercise training schedules. Often long distance runners will have symptoms of Achilles tendonitis after increasing their mileage or increasing the amount of hill training they are doing. As people age, tendons, like other tissues in the body, become less flexible, more rigid, and more susceptible to injury. Therefore, middle-age recreational athletes are most susceptible to Achilles tendonitis.
Symptoms
Mild ache in the back of the lower leg, especially after running. More acute pain may occur after prolonged activity, Tenderness or stiffness in the morning. In most cases the pain associated with Achilles tendinitis is more annoying than debilitating, making sufferers regret activity after the fact, but not keeping them from doing it. More severe pain around the Achilles tendon may be a symptom of a much more serious ruptured tendon.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
As with all conditions, your Doctor should be consulted. Even minor symptoms can represent significant damage to the Achilles tendon. It is recommended that medical advice be sought as soon as symptoms are experienced. Applying ice to the injury on a regular basis can reduce inflammation associated with Achilles Tendonosis. Following the initial injury, ice should be applied for periods of 15 minutes every hour. Resting the injured ankle may be necessary. This can be a problem for athletes who need to train regularly. The degree of rest required depends on the severity and type of Achilles Tendonosis. Your Health Care Professional will advise you about what activities should be limited while the injury is repairing. Fast uphill and downhill running is not advised while an Achilles Tendinosis injury is healing. Anti-inflammatory, analgesic medications such as those containing aspirin may help control pain and inflammation. Self-massage with heat-inducing creams and liniments may be of assistance. Wearing heel-lifts or pads in shoes can reduce the tension in the Achilles tendon. Physiotherapy may assist in the repair of a damaged Achilles tendon. Physiotherapists may recommend exercises to strengthen the tendon to reduce the chances of future injury. Regular stretching of the hamstring muscles (at the back of the calf) can help the repair process. This should only be done when the injury has repaired enough not to cause pain during this stretching. Taping the ankle and wearing appropriate running shoes may help to control movement in the ankle and prevent further injury.
Surgical Treatment
Chronic Achilles tendon tears can be more complicated to repair. A tendon that has torn and retracted (pulled back) into the leg will scar in the shortened position over time. Restoring normal tendon length is usually not an issue when surgery is performed within a few weeks of the injury. However, when there has been a delay of months or longer, the treatment can be more complicated. Several procedures can be used to add length to a chronic Achilles tear. A turndown procedure uses tissue folded down from the top of the calf to add length to the Achilles tendon. Tendon transfers from other tendons of the ankle can also be performed to help restore function of the Achilles. The results of surgery in a chronic situation are seldom as good as an acute repair. However, in some patients, these procedures can help restore function of a chronically damaged Achilles.
Prevention
Suggestions to reduce your risk of Achilles tendonitis include, icorporate stretching into your warm-up and cool-down routines. Maintaining an adequate level of fitness for your sport. Avoid dramatic increases in sports training. If you experience pain in your Achilles tendon, rest the area. Trying to ?work through? the pain will only make your injury worse. Wear good quality supportive shoes appropriate to your sport. If there is foot deformity or flattening, obtain orthoses. Avoid wearing high heels on a regular basis. Maintaining your foot in a ?tiptoe? position shortens your calf muscles and reduces the flexibility of your Achilles tendon. An inflexible Achilles tendon is more susceptible to injury. Maintain a normal healthy weight.
Coping With Pes Planus
Overview

Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy). Unlike a flexible flatfoot, a rigid flatfoot is often the result of a significant problem affecting the structure or alignment of the bones that make up the foot's arch. Some common causes of rigid flatfeet include. Congenital vertical talus. In this condition, there is no arch because the foot bones are not aligned properly. In some cases, there is a reverse curve (rocker-bottom foot, in which the shape is like the bottom rails of a rocking chair) in place of the normal arch. Congenital vertical talus is a rare condition present at birth. It often is associated with a genetic disorder, such as Down syndrome, or other congenital disorders. The cause is unknown in up to half of cases. Tarsal coalition (peroneal spastic flatfoot). In this inherited condition, two or more of the foot bones are fused together, interfering with the flexibility of the foot and eliminating the normal arch. A rare condition, it often affects several generations of the same family. Lateral subtalar dislocation. Sometimes called an acquired flatfoot, it occurs in someone who originally had a normal foot arch. In a lateral subtalar dislocation, there is a dislocation of the talus bone, located within the arch of the foot. The dislocated talus bone slips out of place, drops downward and sideways and collapses the arch. It usually occurs suddenly because of a high-impact injury related to a fall from a height, a motor vehicle accident or participation in sports, and it may be associated with fractures or other injuries.
Causes
Most cases of flatfeet are simply the result of normal development. When that is not the case, the condition can be caused by a number of factors, including the following, Age, disease, injury, obesity or being overweight, physical abnormality, pregnancy. Flattened arches in adults may result from the stresses of aging, weight gain, and the temporary increase in elastin (protein in connective tissue) due to pregnancy. In some cases, flatfeet are caused by a physical abnormality, such as tarsal coalition (two or more bones in the foot that have grown together) or accessory navicular (an extra bone along the side of the foot). The effects of diseases such as diabetes and rheumatoid arthritis can lead to flatfeet. An injury (e.g., bone fracture, dislocation, sprain or tear in any of the tendons and ligaments in the foot and leg) also can cause flatfeet.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
Non Surgical Treatment
The treatment your podiatrist recommends will depend upon the trouble and pain you?re experiencing. Custom shoe inserts (orthotics) are most often recommended and are quite effective. Stretching exercises to loosen and strengthen the supporting tendons may also be recommended. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may recommend an ankle brace or a custom orthotic device that fits into your shoe to support the arch. A short-leg cast or boot may be worn to immobilize the foot and allow the tendon to heal. Ultrasound therapy and stretching exercises may help rehabilitate the tendon and muscle following immobilization. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Your foot and ankle surgeon may recommend changes in your footwear.
Surgical Treatment

Surgical procedures for flat feet vary depending on the root cause of the condition. Surgical correction to control pronation may include bone implants or Achilles tendon lengthening. Tendon transfer, which is a procedure to re-attach a tendon to another area of bone, may also be used to reduce pronation and improve foot function.
Flexible flatfeet are considered normal in young children because babies are not born with a normal arch. The arch may not form fully until sometime between ages 7 and 10. Even in adulthood, 15% to 25% of people have flexible flatfeet. Most of these people never develop symptoms. In many adults who have had flexible flatfeet since childhood, the missing arch is an inherited condition related to a general looseness of ligaments. These people usually have extremely flexible, very mobile joints throughout the body, not only in the feet. Flatfeet also can develop during adulthood. Causes include joint disease, such as rheumatoid arthritis, and disorders of nerve function (neuropathy). Unlike a flexible flatfoot, a rigid flatfoot is often the result of a significant problem affecting the structure or alignment of the bones that make up the foot's arch. Some common causes of rigid flatfeet include. Congenital vertical talus. In this condition, there is no arch because the foot bones are not aligned properly. In some cases, there is a reverse curve (rocker-bottom foot, in which the shape is like the bottom rails of a rocking chair) in place of the normal arch. Congenital vertical talus is a rare condition present at birth. It often is associated with a genetic disorder, such as Down syndrome, or other congenital disorders. The cause is unknown in up to half of cases. Tarsal coalition (peroneal spastic flatfoot). In this inherited condition, two or more of the foot bones are fused together, interfering with the flexibility of the foot and eliminating the normal arch. A rare condition, it often affects several generations of the same family. Lateral subtalar dislocation. Sometimes called an acquired flatfoot, it occurs in someone who originally had a normal foot arch. In a lateral subtalar dislocation, there is a dislocation of the talus bone, located within the arch of the foot. The dislocated talus bone slips out of place, drops downward and sideways and collapses the arch. It usually occurs suddenly because of a high-impact injury related to a fall from a height, a motor vehicle accident or participation in sports, and it may be associated with fractures or other injuries.
Causes
Most cases of flatfeet are simply the result of normal development. When that is not the case, the condition can be caused by a number of factors, including the following, Age, disease, injury, obesity or being overweight, physical abnormality, pregnancy. Flattened arches in adults may result from the stresses of aging, weight gain, and the temporary increase in elastin (protein in connective tissue) due to pregnancy. In some cases, flatfeet are caused by a physical abnormality, such as tarsal coalition (two or more bones in the foot that have grown together) or accessory navicular (an extra bone along the side of the foot). The effects of diseases such as diabetes and rheumatoid arthritis can lead to flatfeet. An injury (e.g., bone fracture, dislocation, sprain or tear in any of the tendons and ligaments in the foot and leg) also can cause flatfeet.
Symptoms
Arches can be seen as ?rolling downward? or collapsing when walking. Pain may present in lower back, hips or knees. Pain may be present on the bottom of the heels, within the arch, within the ankles or even the forefoot. Swelling can occur. Pain may occur in the anterior leg muscles.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
Non Surgical Treatment
The treatment your podiatrist recommends will depend upon the trouble and pain you?re experiencing. Custom shoe inserts (orthotics) are most often recommended and are quite effective. Stretching exercises to loosen and strengthen the supporting tendons may also be recommended. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may recommend an ankle brace or a custom orthotic device that fits into your shoe to support the arch. A short-leg cast or boot may be worn to immobilize the foot and allow the tendon to heal. Ultrasound therapy and stretching exercises may help rehabilitate the tendon and muscle following immobilization. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Your foot and ankle surgeon may recommend changes in your footwear.
Surgical Treatment
Surgical procedures for flat feet vary depending on the root cause of the condition. Surgical correction to control pronation may include bone implants or Achilles tendon lengthening. Tendon transfer, which is a procedure to re-attach a tendon to another area of bone, may also be used to reduce pronation and improve foot function.